This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Vascular dementia may present with language disorders due to damage to frontal subcortical circuits. This study aimed to review recent studies of language abilities in patients with vascular dementia. Sixty-nine studies were classified according to language modalities (spontaneous speech, auditory comprehension, repetition and naming). First, spontaneous speech was impaired in the ability to describe pictures, objects and in the ability to convey information in discourse. Second, the auditory comprehension was impaired in word comprehension, sentence comprehension, paragraph comprehension, and speech act comprehension tasks. Third, repetition was preserved in word-level tasks but impaired at the sentence level. Fourth, the naming performance was impaired in a generative naming task (phonemic fluency) rather than in a confrontational naming task. Therefore, when summarizing the results between patient groups, in spontaneous speech, to convey information through highly informative utterances was relatively good in vascular dementia (VaD), but the number of utterances was lower than dementia of Alzheimer’s type (DAT). In auditory comprehension, VaD’s performance was good in the task of word comprehension and speech act comprehension tasks. It is organized as in repetition, VaD’s performance was relatively good in the sentence-level task, and in naming, VaD’s performance was reported to be better than DAT in the oppositional naming and generative naming semantic category tasks. In the generative naming phoneme category, opposite result was reported. Further studies on the language abilities of patients with vascular dementia needs to consider factors such as subtype and language modality. Future studies should be evenly distributed across all language domains.
치매는 다양한 원인 질환으로 인하여 다발성 인지기능장애를 보이며 일상생활 능력이 저하된 상태를 말한다. 우리나라는 현재 65세 이상의 치매 환자가 984,601명으로 산정되며 이는 전체 노인 인구 중 10.41%를 차지한다(Central Dementia Center, 2023). 국외 치매 환자 현황의 경우, 치매 유형 중 알츠하이머성 치매(dementia of Alzheimer’s type, DAT)가 가장 빈번하고 혈관성 치매(vascular dementia, VaD)가 그 뒤를 이어 두 번째로 흔하게 나타나는 것으로 보고된다(Dubois & Hébert, 2001). 그러나 국내 치매 환자 현황을 살펴보면 DAT가 약 75.5%로 가장 많고, 기타 유형의 치매가 15.5%로 그 뒤를 따르며 VaD가 8.6%로 세 번째로 많이 나타나는 것으로 보고된다(Central Dementia Center, 2022). 따라서 국외와 국내 모두에서 VaD 환자가 많이 분포함을 알 수 있다. VaD는 뇌로 가는 혈류가 감소하거나 뇌혈관이 터지는 등의 뇌졸중을 포함한 다양한 뇌혈관 질환(cerebrovascular disease)으로 인하여 발생하며, 뇌혈관 질환의 주요 위험요인으로는 고혈압, 당뇨, 고지혈증, 고콜레스테롤혈증 등의 대사증후군이 손꼽힌다(Gupta et al., 2005). 우리나라에서 뇌졸중은 단일 질환 중 가장 흔한 질환에 해당되며(Korean National Statistical Office, 2000), 우리나라를 비롯한 동양권에서는 과도한 염분 섭취 등의 식습관으로 인하여 위에서 언급한 뇌혈관 질환의 위험에 크게 노출되어 있기 때문에 서양권과 비교하여 특히 VaD의 유병률이 높다(Ikeda et al., 2001). 따라서 뇌혈관 질환으로 인하여 인지기능장애와 더불어 일상생활 능력의 장애까지 야기시킬 수 있으므로 DAT만큼 VaD에 대해 주목할 필요가 있다.
경도인지장애(mild cognitive impairment, MCI)는 정상적인 노화와 초기 치매 사이의 인지 변화를 의미하는 과도기적인 단계의 인지기능장애를 뜻하며, 인지적 기능은 저하되었으나 일상생활 능력에서의 저하를 보이지 않는다는 특징이 있다(Petersen et al., 1999). 또한 빠른 시기에 발견하여 중재할 경우 그 효과가 커질 수 있다고 알려져 있으므로 MCI 증상이 나타나는 환자들의 특성을 파악하는 것도 중요하다(Roh & Park, 2019). MCI는 장애가 나타나는 인지 영역이 무엇인지에 따라 기억상실형 경도인지장애(amnestic MCI, aMCI)와 비기억상실형 경도인지장애(non-amnestic MCI, naMCI)로 분류되는데, naMCI 환자들은 향후 VaD 또는 전두측두엽치매와 같은 치매 질환으로 진행될 가능성이 높은 것으로 알려져 있다(Roh & Park, 2019). 치매로의 이환율을 살펴보면, 약 80%의 MCI 환자가 6년 안에 치매 증상을 보이는 것으로 보고된 연구가 있으며(Peterson et al., 2001) 그중 DAT가 아닌 다른 치매로 발전할 위험도가 17.6%로 보고되었다(Meyer et al., 2002). 따라서 치매로의 이환율이 높은 경도인지장애 중에서 뇌혈관 질환 발생 부위에 따라 다양한 임상 증상이 나타나는 혈관성 질환이 있는 MCI 환자의 언어 능력을 살펴보는 것도 중요하다.
증상이 점진적으로 발생하는 DAT와는 달리 VaD는 증상의 발생이 다소 급작스럽게 발생하고 계단식으로 악화된다고 보고된다(Van Straaten et al., 2003). 신경심리검사 상에서 기억력, 이름대기, 시공간능력의 손상이 초기부터 두드러지는 DAT와 다르게 VaD는 주로 전두엽-집행기능장애가 두드러지고 특히 인출(retrieval) 능력의 손상이 심하게 나타나는 것으로 알려져 있다(O’Brien, 2003; O’Brien & Thomas, 2015; Stebbins et al., 2008). 그러나 VaD의 발병, 경과 및 예후는 원인이 되는 뇌혈관 질환에 영향을 받기 때문에 질환의 유형, 병소의 위치와 크기에 따라 다양한 양상을 보일 수 있고 아형에 따라 매우 이질적일 수 있다(Korczyn, 2002; Loeb & Meyer, 1996). 미국 국립 신경질환 및 뇌졸중 협회와 국제 신경과학 연구 및 교육 협회(National Institute of Neurological Disorders and Stroke-Association International pour la Recherche et l’Enseignement en Neurosciences, NINDS-AIREN)에서는 NINDS-AIREN의 기준에 근거하여 VaD를 1) 피질 또는 피질과 피질하 영역에 동시에 병변을 보이는 다발성 뇌경색 치매(multi-infarct dementia, MID), 2) 소동맥 질환(small vessel disease)에 의해 유발된 피질하 영역의 다발성 열공경색이나 심한 백질변성으로 인하여 피질하 영역에 병변을 보이는 피질하 혈관성 치매(subcortical VaD, SvaD), 3) 특정 뇌 부위의 단일 경색으로 치매 증상이 발생하는 전략적 뇌경색 치매(strategic infarct dementia), 4) 심정지 등 후에 나타나는 저관류에 의한 치매(hypoperfusion dementia), 5) 뇌출혈로 인한 출혈성 치매(hemorrhagic dementia), 6) 피질하 뇌경색과 백질뇌증을 동반하는 상염색체 우성 뇌동맥 질환으로 나타나는 유전성 혈관성 치매(hereditary VaD [cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy, CADASIL]), 7) 알츠하이머성 치매와 혈관성 치매의 혼합형(Alzheimer’s disease with cardiovascular disease)으로 분류하였다(Farooq & Gorelick, 2013; Hachinski et al., 2006; O’Brien & Thomas, 2015; Román et al., 1993). 위와 같은 혈관성 병리가 주로 나타나는 병소 부위는 다음과 같다: 1) 언어-인지와 관련된 주요 뇌 영역에 혈액을 공급하는 중대뇌동맥을 포함한 윌리스환의 주요 동맥 경색(Brun, 1994; Thal et al., 2012), 2) 피질하 백질 영역 동맥의 말단 부분 경색(Giwa et al., 2012; Ho & Garcia, 2000; Wardlaw, 2010), 3) 전두엽, 시상, 기저핵과 같은 특정 부위의 경색(Jellinger, 2013), 4) 전, 중, 후대 뇌동맥이 담당하는 구역의 경계에서 발생하는 경계구역경색(watershed infarction)과 피질층상괴사(cortical laminar necrosis) (Jellinger, 2013; Johnston et al., 2004; Marshall, 2012), 5) 혈관 주위 또는 뇌엽과 기저핵의 출혈(Charidimou et al., 2012; Henskens et al., 2008), 6) 피질하 백질이나 기저핵의 변성(Chabriat et al., 2009; Federico et al., 2012; Keverne et al., 2007; Schmidt et al., 2012), 7) 아밀로이드 병리와 백질 병변(열공경색)의 동반(Jellinger, 2013; Thal et al., 2012). 이러한 병소 부위는 다양한 인지기능장애를 유발할 수 있으나 대체로 VaD 환자는 초기부터 전두엽 및 전두엽-피질하 회로의 결함과 관련이 있는 전두엽 집행기능장애를 보이므로(Desmond, 2004) 진단을 위하여 정보 처리 속도, 복잡한 주의력 및 전두엽 집행 기능에 중점을 두는 지침이 소개되었다(Sachdev et al., 2014).
전두엽-피질하 회로(frontal-subcortical circuit)는 전두엽과 더불어 피질하 구조물인 기저핵과 시상으로 구성된다. 전두엽은 일차운동영역(primary motor area), 전두안구영역(frontal eye field), 배외측전전두피질(dorsolateral prefrontal cortex), 전대상회(anterior cingulate gyrus), 안와전두피질(orbitofrontal cortex)로 나누어져 있으며, 각 영역에서 시작된 정보가 기저핵과 시상을 거쳐 다시 대뇌피질로 투사되는 되먹임 경로(feedback pathway)를 이룬다. 전두엽-피질하 회로는 크게 운동을 조절하는 운동 회로, 비운동 회로로 나뉘는데 먼저 운동 회로는 일차운동영역에서 시작된 정보가 운동 회로(motor circuit)를 통해 사지운동을 조절하며, 전두안구영역에서 시작된 정보는 안구운동 회로(oculomotor circuit)를 통해 안구운동을 조절한다. 비운동 회로는 배외측전전두피질에서 시작된 정보가 배외측전전두피질 회로(dorsolateral prefrontal circuit)를 통해 집행기능, 작업기억, 판단력 등 고도의 인지기능을 조절하며, 전대상회에서 시작된 정보는 전대상회 회로(anterior cingulate circuit)를 통해 동기를 조절하고, 안와전두피질에서 시작된 정보는 안와전두피질 회로(orbitofrontal circuit)를 통해 충동 억제를 조절한다(Cummings, 1998).
이 중 인지기능을 조절하는 배외측전전두피질 회로가 손상되면 계획 및 조직화 능력의 저하, 심리운동적 느림, 집행기능장애 등을 뚜렷한 특징으로 나타내는데(Looi & Sachdev, 1999), 이러한 전두엽-집행기능장애는 언어 과제의 수행에도 부정적인 영향을 미칠 수 있다. 그러나 VaD의 언어 능력에 대해서는 구어유창성 과제의 수행력 저하를 보고한 연구(Kertesz & Clydesdale, 1994)를 제외하고는 VaD의 말과 언어 영역을 구분 짓지 않고 총괄적으로만 정리하고 있거나(Ross et al., 1990), DAT에 초점을 둔 연구에서 대조군으로서 VaD의 언어 능력을 다루는 경우가 주를 이루었다(Vuorinen et al., 2000). 인지와 언어 능력의 유기적인 관계에 따라 각 치매 유형에서 나타나는 언어 특성을 이해하는 것은 매우 중요하지만(Assal & Ghika, 2013), VaD의 높은 유병률에 비하여 이들의 언어 특성에 초점을 둔 문헌 연구는 전무하기 때문에 DAT에 비해 알려진 바가 적다(Sellal et al., 2004). 이에 본 연구에서는 VaD를 대상으로 언어 능력을 살펴본 국내외 문헌들을 고찰하고 그 결과를 종합함으로써 VaD의 언어 특성을 파악하고자 한다.
MATERIALS AND METHODS
문헌 수집 및 선정
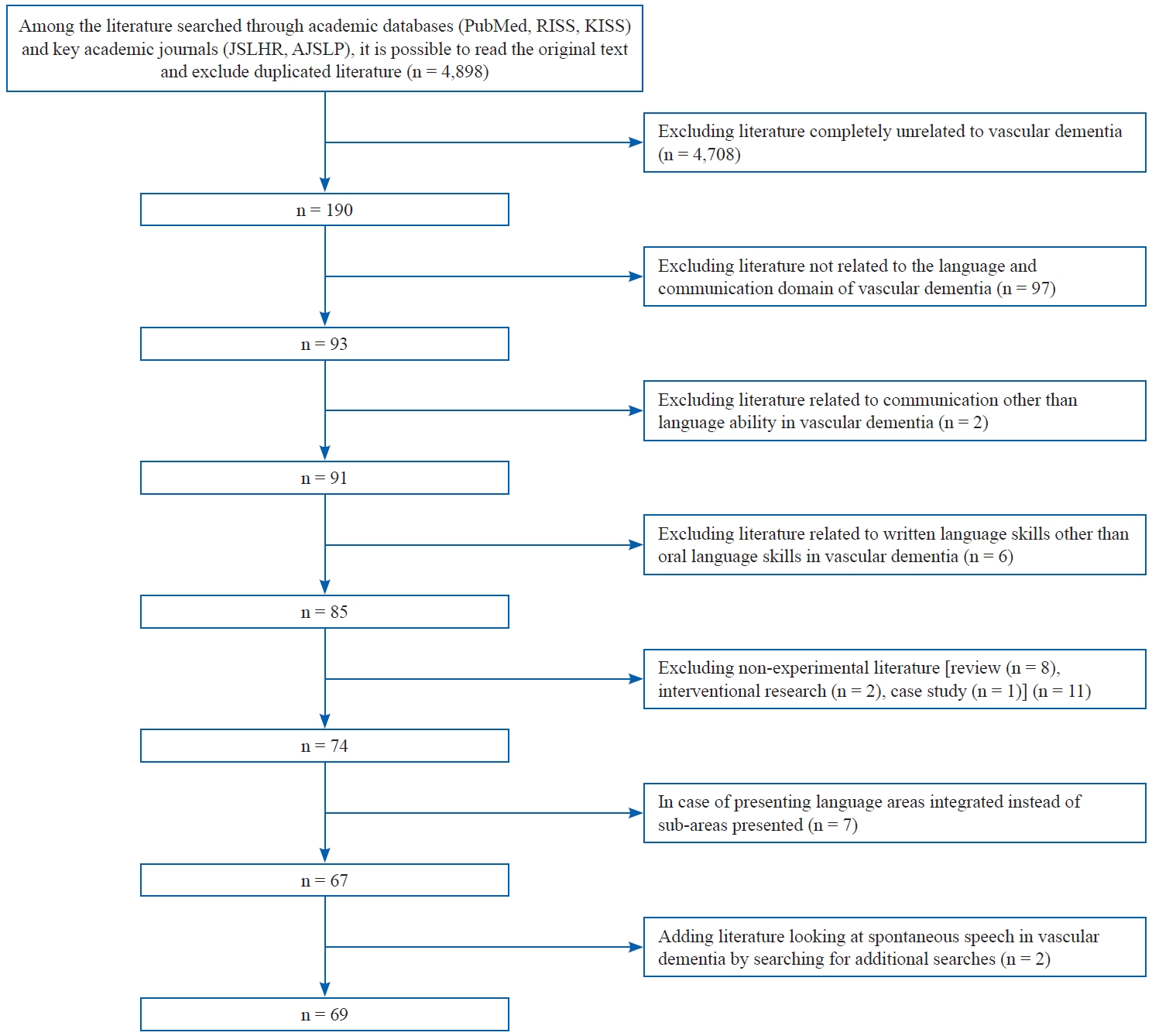
문헌 분석을 위하여 1959년도 1월 1일부터 2023년 4월 30일까지 발간된 자료로 한정하였다. 국외 문헌의 경우 미국 국립의학도서관의 검색엔진인 ‘PubMed’와 언어병리학 학술지인 ‘Journal of Speech, Language, and Hearing Research’, ‘American Journal of Speech Language Pathology’를 통하여 문헌을 수집하였다. 핵심어로는 ‘vascular, language, linguistic, spontaneous speech, comprehension, repetition, naming’을 조합하였다. 국내 문헌의 경우 학술연구정보서비스(RISS)와 한국학술정보(KISS)를 통하여 문헌을 수집하였다. 핵심어로는 ‘혈관, 언어, 스스로 말하기, 자발화, 이해, 알아듣기, 따라말하기, 명명하기, 이름대기’ 등의 용어를 조합하였다. 검색 시 원문 열람이 가능하고 영어와 한국어로 작성된 문헌 중 중복된 문헌을 제외한 결과, 총 4,898편에서 다음 단락의 선정 기준에 따라 67편의 문헌이 선정되었으며 개별 검색을 통하여 2편이 더 추가되어 최종적으로 69편이 분석 논문으로 선정되었다.
문헌 포함 및 제외 절차
선정된 문헌에 대하여 모든 저자는 상호 의논 및 합의를 통하여 다음과 같은 포함 및 제외 기준을 결정하였다. 구체적인 문헌 선정 기준은 (1) VaD와 전혀 관련이 없는 문헌은 제외하며, 그중 (2) VaD의 언어 및 의사소통 영역과 관련이 없는 문헌을 제외하였고, 다음으로 (3) 언어 능력이 아닌 기타 의사소통 분야(예: 말, 삼킴 등)에 해당하는 문헌은 제외하였으며, (4) 언어 능력 중 구어 능력이 포함되지 않은, 문어(읽기, 쓰기) 능력에 대해서만 제시된 문헌은 제외하였다. 또한 (5) 실험 연구가 아닌 문헌(예: 종설, 중재 연구, 사례 연구 등)을 제외하였고 (6) 종합신경심리검사 중하위 영역별로 제시하지 않고 언어 영역을 통합하여 제시한 경우는 제외하였다(Figure 1). 상기 포함 및 제외 기준에 따라 문헌을 분류할 시, 연구자들 간의 의견 불일치는 발생하지 않았다.
문헌 분석을 위하여 대상자의 구성을 확인한 결과, 전체 문헌 69편 중 VaD의 아형을 구분하지 않고 다룬 문헌이 44편, VaD의 아형을 구분한 문헌이 25편이었다. 이에 연구 결과에서는 전반적인 VaD 대상으로 진행된 연구의 결과를 먼저 기술한 후에, VaD 아형에 따른 특징적인 연구 결과를 추가적으로 기술하는 방식을 사용하였다. 결과 분석 시에는 신경학적 손상으로 인한 언어장애인의 진단 및 중재의 기초가 되는 언어양식(language modality)의 분류에 따라 자발화(스스로 말하기), 알아듣기, 따라말하기, 이름대기의 4가지 측면에서 각 특성을 구분하여 기술하였다.
RESULTS
VaD의 언어 특성
자발화
자발화는 자발적으로 구어를 산출하는 능력이며 임상 상황에서 설명하기나 이야기하기 등의 다양한 발화 유도 과제를 사용하여 평가한다. VaD의 자발화를 살펴본 연구는 총 11편이었다(Table 1).
다양한 담화 과제(이야기 담화, 절차적 담화, 일화적 담화, 대화적 담화, 설명적 담화)를 통한 VaD 담화 능력을 DAT와 비교한 결과, 전체 발화 수는 VaD가 적었으나 담화의 주제에 대해 적절하고 정보성 높은 발화를 사용함으로써 정보 전달 능력이 높게 나타났다(Son & Park, 2008). 전체 발화 수 중에서 주제유지가 된 발화의 비율을 살펴보는 주제유지 능력의 경우, 두 집단이 유사하였으며 모두 전체 발화의 50% 정도의 주제유지 능력을 보이고 있는 것으로 나타났다. 그리고 담화 내의 결속표지 사용 빈도에서도 비슷한 정도를 보였다(Son & Park, 2008). 또한 VaD 집단 내에서 중증도별로 살펴보았을 때 치매 초기에는 결속표지의 사용 빈도가 증가하나 치매의 증상이 심해질수록 결속 표지의 사용이 줄어들었다(Son & Park, 2012).
VaD의 특정 아형을 대상으로 진행된 연구를 살펴보면, MID의 경우 자발적인 구어 산출에서 DAT보다 더 많은 정보를 가지는 것으로 나타났다(Powell et al., 1988).
알아듣기
알아듣기는 청각적으로 제시된 말을 듣고 그 뜻을 이해하는 능력이다. 과제를 언어학적 단위의 측면으로 분류할 때, 단어 수준의 알아듣기 능력은 청각적 낱말 인지 과제를 사용하고, 문장 수준의 알아듣기 과제의 경우 질문 이해와 명령 이해 과제를 사용하며, 문단 수준의 알아듣기 과제는 이야기 이해, 정의에 대한 이해, 화행 이해를 통해 평가한다. 알아듣기를 살펴본 연구는 총 17편이었다(Table 2).
VaD의 문단 수준 알아듣기 능력을 살펴보았을 때, 이야기 이해 과제의 경우 연구의 대상에 VaD와 DAT만 포함되어, HC와 비교한 결과는 찾을 수 없었으며(Yeo & Kim, 2020), DAT보다 VaD의 수행력이 저하되는 것으로 나타났다(Yeo & Kim, 2020). 반면에, 한 문장 이상으로 이루어진 단어의 정의를 듣고 적절한 그림을 찾는 과제를 실시한 연구에서는 DAT보다 VaD의 수행력이 높았다(Oh et al., 2010). 화행의 유형(단언형, 지시형, 언약형, 표현형, 선언형)에 따라 발화의 의도를 이해하는지 알아보기 위해 시나리오를 청각적으로 제시하고 시나리오의 언표 내적 의미를 이해한 후 4개의 보기 문항 중 적절한 반응을 고르는 과제로 살펴본 화행 이해 능력의 경우, HC와 비교하였을 때 VaD의 수행력이 저하되는 것으로 나타났으며, 환자군 간 비교한 결과, DAT보다 VaD의 수행력이 높았다(Kim & Sin, 2014).
추가적으로 VaD의 특정 아형을 대상으로 진행된 연구를 살펴보면, SVaD의 경우 청각적 낱말 인지 과제에서 HC, DAT 모두와 유의미한 차이가 나타나지 않는 것으로 보고되었다(Graham et al., 2004). 문장을 듣고 토큰을 활용하여 수행하는 토큰 검사에서는 HC보다 수행력이 저하되는 것으로 보고되었으며, 환자군 간 비교하여 살펴보면, DAT와 유사한 수행력을 보였다(Cannatà et al., 2002; Traykov et al., 2002). 이외, 신경심리학검사에 포함된 알아듣기 및 이해력 검사를 실시한 결과, HC와 비교하여 SvaD의 수행력이 저하된다는 보고(Cohen et al., 2002)와 차이가 나타나지 않는다는 연구가 함께 나타났다(Matioli & Caramelli, 2012). 수행력의 차이가 나타난 것으로 밝혀진 연구는 피질하만 손상된 경우가 피질과 피질하 모두에 손상이 있는 경우보다 수행력이 좋은 것으로 보고하였다(Cohen et al., 2002). 신경심리학검사에서 알아듣기 및 이해력 검사를 환자군 간에서 비교한 연구의 경우 DAT의 수행력이 SvaD보다 높았다(Han et al., 2006). MID의 경우, 명령이행 능력에서 HC보다 어려움이 있는 것으로 나타났으며, 환자군 내의 비교에서는 5년 이상의 비정상적 혈압이나 동맥경화증 같은 혈관 질환의 병력은 가지고 있으나 뇌경색은 없었던 집단이 MID보다 수행력이 높은 것으로 보고되었다(Emery et al., 1996).
따라말하기
따라말하기는 청각적으로 제시된 단어나 문장을 듣고 구두로 모방하는 능력이다. 따라말하기를 살펴본 연구는 총 6편이었다(Table 3). 단어 수준에서 VaD는 HC 및 DAT와 비교하여 따라말하기 능력에 차이가 없었으나, 문장 수준에서는 DAT보다는 수행력이 높았으나 HC보다 저하되었으며(Freitas et al., 2018; Vuorinen et al., 2000) VaD의 전임상적 단계인 vMCI 단계에서부터 HC보다 저하되는 수행력이 관찰되었다(Nordlund et al., 2007).
VaD의 하위 유형 중 SvaD의 경우, HC와 DAT와의 수행력 차이가 없는 것으로 보고되었다(Han et al., 2006; Matioli & Caramelli, 2012). 또한 하위 유형 중 MID는 HC와 차이가 나타나지 않았으나 단일 경색 집단은 HC에 비해 수행력이 저하되었다(Emery et al., 1996).
CADASIL 환자를 대상으로 대면이름대기, 손가락 이름대기, 생성이름대기 능력을 살펴본 문헌(Peters et al., 2005)에서는 대면이름대기와 손가락 이름대기는 HC와 비교하여 차이가 없었으나, 생성이름대기 능력은 CADASIL의 수행력이 저하되었다.
DAT와 VaD의 혼합형 환자를 대상으로 청각적으로 제시된 단어의 정의를 듣고 이름대기를 하는(예: 왕이 머리에 쓰는 것) 청각적 이름대기 능력과 대면이름대기 능력을 살펴본 문헌(Hirsch et al., 2021)에서는 두 수행력 모두에서 인지기능이 상대적으로 높은 HC, aMCI, naMCI에 비해 DAT와 VaD의 혼합형과 VaD가 저하되는 소견을 보였다. 그러나 DAT와 VaD의 혼합형과 VaD 간의 유의미한 수행력 차이는 나타나지 않았다.
DISCUSSIONS
본 연구는 국내외에서 VaD의 언어 능력을 살펴본 69편(Appendix 2)의 문헌을 분석하여 언어의 하위 양식에 따라 자발화, 알아듣기, 따라말하기, 이름대기로 구분하여 결과를 제시하였다. 대부분의 문헌에서는 VaD의 언어 특성을 확인하기 위하여 DAT와 비교하였다. 언어 영역별 결과를 종합해보면, VaD 환자는 자발화 능력의 경우 적절한 의도를 포함한 정보성 높은 발화에 따른 정보 전달 능력이 좋으나 발화의 수는 DAT보다 적게 나타났다. 알아듣기 능력의 경우, 이야기 이해에서 VaD의 수행력이 다소 저하되는 것으로 나타났으나, 단어의 정의를 듣고 적절한 그림을 찾는 과제 및 발화의 의도를 이해하여 응답하는 화행 이해 과제의 경우 VaD의 수행력이 좋은 것으로 정리된다. 따라말하기 능력의 경우, 문장 수준 과제에서 VaD의 수행력이 비교적 좋게 나타났으며, 이름대기 능력에서 대면이름대기와 생성이름대기 의미범주 과제에서 VaD의 수행력이 DAT보다 좋은 것으로 다수 보고되었으며 생성이름대기 음소범주에서는 그 반대의 결과가 보고되었다. 이에 대한 논의는 다음과 같다.
자발화
임상에서 자발화 능력은 설명이나 이야기하기 등의 담화 과제로 평가될 수 있으며 이를 통해 전반적인 어휘 및 의미, 형태 및 구문, 화용 능력을 각각 살펴볼 수 있다. VaD와 DAT를 비교하여 발화 능력을 살펴보았을 때, 어휘 및 의미 영역에서 VaD는 내용상 적절하고 올바른 정보를 제공하는 어절 산출의 빈도 수가 DAT에 비하여 비교적 높게 나타났다(Son & Park, 2008). 그러나 형태 및 구문 영역에서는 구문 복잡성이 저하되면서 DAT보다 단순한 문장을 산출하였고 산출된 전체 발화 수나 단어의 수가 적었다(Hier et al., 1985). 이러한 결과는 VaD의 신경병리적 특성과 관련이 있을 수 있다. 형태소의 활용이나 구문 산출의 기능은 전두엽에서 주로 담당하는데, VaD는 비교적 정보를 등록하고 보유하는 측두엽의 기능은 유지되기 때문에 어휘-의미적으로는 적절한 내용어에 접근할 수 있었으나 형태소의 활용이나 구문 산출과 관련이 있는 전두엽의 기능이 저하되므로 저장된 정보를 산출하는 구문적 처리 과정에서 이상을 보일 수 있다(Taylor et al., 1990).
한편, 화용은 언어가 어떤 목적으로 사용되는지에 관심을 가지며, 화자가 발화하는 ‘의도된 기능, 즉 발화수반력’, ‘언어적 형태, 즉 발화’, ‘청자에 미치는 영향, 즉 발화 효과’로서 이 세 가지 요소로 구성된다. 따라서 ‘의도’, ‘형태’, ‘효과’ 요소의 맥락에서 VaD의 화용 능력을 살펴보면, DAT에 비하여 VaD의 발화 수반 행위에 나타나는 화자의 ‘의도’가 충분히 포함되어 청자에게 적절한 내용의 정보를 전달하는 능력, 즉 발화 ‘효과’가 좋은 편이나 ‘형태’ 요소의 경우, DAT보다 VaD의 전체 발화 수의 평균 값이 상대적으로 낮게 나타나게 되어 VaD가 언어적 형태를 활용하여 충분히 발화를 산출하는 것에는 어려움을 가지는 것으로 해석해 볼 수 있다.
그리고 이렇게 화용적 측면에서 본인의 의도를 잘 전달하기 위해서는 발화의 주제를 유지하는 능력 또한 필수적인데, 이러한 능력은 미시적 관점에서의 언어의 어휘 및 의미, 형태 및 구문 능력과 더불어 거시적 관점에서 낱말 간의 유기적인 결합으로 구성된 문장들이 서로 연관성을 가지고 통일된 내용으로 응집되면서 주제와 관련 있는 정보를 유지하고 개념을 통합하는 능력을 요구한다(Burke & Shafto, 2011). Son & Park(2008)의 연구에서는 VaD와 DAT 집단 간 주제유지 측면에서 유의미한 차이가 나타나지 않았으며 VaD와 DAT 모두 산출한 전체 발화의 수 중에서 주제유지가 가능하였던 발화가 50% 정도로만 나타나 주제 유지 능력이 전반적으로 저하되어 있는 것으로 나타났다.
두 환자군에 대한 화용 능력을 살펴본 다른 연구(Laine et al., 1998)에서는 VaD와 DAT 모두 HC에 비하여 전반적 응집성(global coherence) 손상, 즉 모든 문장들 사이의 관계성과 전반적인 주제에 근거한 응집성의 손상 및 정보성 감소가 나타났다. 이는 주제유지 능력에도 어려움을 보이는 Son & Park(2008) 연구의 결과와 유사한 측면을 나타냈다. 그러나 Laine et al.(1998)은 DAT에 비하여 VaD가 발화를 비교적 응집성 있게 산출한다는 결과를 추가로 보고하면서 VaD가 청자에게 더 적절하게 의도를 전달하는 것으로 해석하였다. 이러한 결과는 극초기 및 심도의 환자가 대상자군에 포함되지 않아서 집단 간 차이가 관찰되었을 가능성이 있다. 반면에, 치매의심 단계의 초기 환자부터 말기의 환자까지 모두 포함한 Son & Park(2008) 연구에서는 초기 환자가 보이는 천장효과나 심도 환자가 보이는 바닥효과로 인하여 집단 간 차이가 나타나지 않았을 가능성이 있겠다.
VaD의 하위 유형 중 MID의 경우, DAT 환자와의 비교에서 MID 환자가 단어 산출이 적고 다양성이 낮으며 문장도 짧고 구문론적으로 덜 복잡하다는 특징을 보인다고 보고되었다(Powell et al., 1988). 따라서 VaD의 주제유지 능력의 경우, 손상 영역 및 환자의 중증도에 따라 수행의 차이를 보이지만 아형에 따라 하위 유형을 자세히 알 수 있을 경우 그에 따른 자발화 특징을 확인할 수 있어, VaD의 세부 아형에 따른 특징을 면밀히 살펴볼 필요가 있는 것으로 생각된다.
알아듣기
청각적 이해 능력은 청각적으로 듣고 단순히 선택하거나 단답형(예/아니오)의 구두로 반응하는 양식과 더불어 청각적인 지시를 듣고 행동으로 수행하는 보다 복잡한 수준의 양식으로 확인될 수 있다. 이 중 청각적으로 지시문을 듣고 행동으로 지시를 수행하는 토큰 검사는 문장에 대한 구문적 지식과 더불어 들은 내용을 잠시 보유하고 이를 인지적 행동 조작을 통해 수행해야 하는 과제이기 때문에 알아듣기 능력과 더불어 작업기억의 처리 과정을 동시에 살펴볼 수 있는 특징이 있다(Yeo & Kim, 2020). VaD의 경우, 뇌혈관의 변화가 전두엽에 영향을 주어 집행기능이 저하되고 특히 인지 처리 속도가 느려지게 되며(Román, 1999), 작업기억의 손상이 특징적으로 보고되었다(Villardita, 1993). 따라서 검사자의 지시를 청각적으로 듣고 행동으로 수행하는 과제에서 HC에 비하여 VaD 환자군이 저하된 수행력을 보였을 가능성이 있다.
문단 수준의 글을 듣고 이해하는 능력은 DAT 집단과의 비교를 통해 확인되었는데, 문단 수준의 이야기를 이해하는 능력은 개별 단어나 문장 이해력 이상의 능력을 요구하며 이는 이야기 안의 응집성 및 추론을 통한 일관적인 표상을 확립해야 한다(Lee et al., 1996). 따라서 다양한 처리 과정을 요구하는 이야기 이해 능력은 집행기능과 중요하게 관련되어 있으며 특히 추론 능력은 작업기억 및 언어 유창성 능력과 관련이 있어(Choi, 2015) 전두엽 기능 저하가 특징인 VaD의 어려움이 문단 수준의 이야기 이해 능력에도 반영된 것으로 이해할 수 있다.
VaD의 하위 유형 중 하나인 SVaD를 대상으로 알아듣기 능력을 살펴본 결과, DAT와 SVaD의 수행력 차이가 나타나지 않는 것으로 보고한 연구에서는 청각적 낱말 인지 검사를 실시하였고, SVaD와 DAT가 함께 나타나는 혼합형 치매 환자를 제외하려는 노력에도 불구하고 임상 진단에 대한 신경병리학적인 확인이 부족하여 진단 오분류의 비율에 대해 확신할 수 없다는 제한점을 나타냈다(Graham et al., 2004). 따라서 SVaD로 분류된 집단 내에 혼합형 치매 환자가 포함되었을 수 있는 가능성으로 인해 듣고 이해하는 과제의 수행력에서 환자군 간 유의미한 차이가 발견되지 않은 것으로 해석된다. 그러나 SVaD가 DAT보다 알아듣기 능력이 좋은 것으로 나타난 연구의 경우, SVaD가 DAT보다 언어기능이 좋은 것으로 나타난 선행 연구의 결과와 일치한 것으로 보고하며(Román & Royall, 1999) DAT는 초기부터 최근 기억 저하의 특징 및 언어 문제를 가지게 되어(Chenoweth & Spencer, 1986) 언어적으로 듣고 이해하여 수행하는 알아듣기 과제에 SVaD와의 수행력 차이를 나타내는 것으로 확인된다.
VaD의 하위 유형 중 하나인 MID의 경우, 명령이행 능력에서 HC보다 어려움을 나타냈는데, 반복적인 뇌경색에 의하여 전두엽-집행기능이 뚜렷하게 손상됨에 따라(Kertesz & Clydesdale, 1994) MID 역시 청각적 명령을 듣고 이를 행동으로 이행하는 것에 어려움을 겪는 것으로 해석된다. 이와 더불어 환자군 내의 비교에서는 뇌경색이 없는 집단과 비교하여 MID의 수행력이 가장 저하되는 것으로 보고되었다. 이러한 결과는 MID의 경우, 여러 차례 반복된 뇌경색에 의하여 뇌손상의 병변 및 중증도가 크며(Kertesz & Clydesdale, 1994) 경색된 영역들이 담당하는 보다 다양한 인지기능의 장애가 나타나게 되어(McPherson & Cummings, 1996) 수행력이 저하된 것으로 해석된다.
따라말하기
따라말하기의 수행은 청각적으로 들은 자극을 등록(부호화)하고 잠시 보유(저장)하였다가 회상(인출)하는 일련의 과정을 거친다. VaD가 DAT에 비하여 문장 따라말하기에서 높은 수행력을 보인 것은 VaD가 문장 수준에 대한 언어적 기억 기능에서 그 능력이 어느 정도 유지됨을 보여준다(Reed et al., 2007). 특히 단서(cue)가 주어질 경우 VaD의 기억 회상 수행이 증진(Looi & Sachdev, 1999)되는 결과를 통해 VaD는 기억 과정 중 인출에 어려움이 있지만 등록과 보유에서는 그 장애의 정도가 심하지 않음을 시사한다. 따라서 전반적인 기억 과정의 장애가 두드러지는 DAT가 상대적으로 낮은 수행을 보인 것으로 생각해 볼 수 있다. 그러나 HC에 비해서는 vMCI가 저조한 따라말하기 능력을 보였는데, 이는 집행 능력 저하 및 주의력 저하 등으로 인해 다양한 인지적 검사의 수행과 결과에 영향을 미치기 때문으로 해석하였다(Nordlund et al., 2007).
VaD의 하위 유형 중 하나인 SVaD를 대상으로 따라말하기 능력을 살펴본 결과, HC와 DAT, SVaD의 차이가 없는 것으로 보고한 연구(Han et al., 2006;; Matioli & Caramelli, 2012)도 있고, HC와 SVaD의 수행 차이는 없으나 HC보다 DAT만 수행이 낮은 것으로 보고된 연구도 있었다(Vuorinen et al., 2000). 집단 간 유의하지 않은 결과를 나타낸 Han et al.(2006)의 연구에서는 대상자가 초기 DAT와 초기 SVaD 환자들을 대상으로 하여, 집단 간 차이가 크지 않았을 것으로 해석된다. 따라서 질환이 진행함에 따라 따라말하기 과제의 수행력 변화를 살펴볼 필요성이 있음을 시사한다. 반면 HC와 비교하였을 때 DAT만 유의미한 차이를 나타내며 HC와 SVaD 간 유사한 따라말하기 수행력을 나타낸 Vuorinen et al.(2000) 연구에서는 SVaD도 기억력 손상이 있을 수 있지만 위에서 언급하였듯이 DAT의 경우 전반적으로 기억력 손상이 더 두드러지기 때문에 나타난 결과로 해석하였다. MID의 경우 HC와 따라말하기 수행력의 차이가 나타나지 않았고 단일 경색 환자만이 HC와 유의미한 차이를 나타냈는데, 이는 뇌경색 이후 평균 2.8년의 시간을 보낸 일부 단일 뇌졸중 환자가 마비말장애 증상을 여전히 보여 나타난 결과로 확인된다.
이름대기
VaD의 이름대기 수행력을 살펴본 결과, 대면이름대기 능력은 HC와 비교하여 수행력이 저하되고 DAT와 비교하여서는 수행력이 높았다. 이러한 결과는 대상자의 병리 및 과제의 특성에 따른 차이로 설명할 수 있다. 대면이름대기는 시각적 분석을 통해 사물의 의미가 저장된 어휘체계와 어휘를 산출하는 데 필요한 음운적 형태가 저장된 음운체계를 거쳐 사물의 이름을 산출할 수 있게 되는 단계를 통해 수행된다(Ellis et al., 1988). 이에 대면이름대기 과제는 어휘-의미 능력을 확인할 수 있는 과제로 유용하게 사용되며, 특히 어휘-의미 능력을 담당하는 측두엽의 손상으로 전반적인 인지기능 중 어휘-의미 능력의 장애가 두드러지는 DAT 환자에서 취약할 수 있다(Choi, 2008). 그러나 VaD의 경우 의미기억 자체의 문제가 있기보다는 의미기억에 저장된 어휘 목록에서 의미 또는 음소범주에 적절한 어휘를 선택하여 인출하는 과정 상의 문제가 있고(Chertkow & Bub, 1990), 생성이름대기에 더 취약할 수 있다, 특히 생성이름대기 내에서도 의미범주보다 음소범주의 수행력이 저하되는 양상은 의미범주의 이름대기가 어휘-의미기억을 담당하는 측두엽과 더 연관되나, 음소 범주의 이름대기는 어휘-음운기억을 담당하는 전두엽과 더 연관되기 때문으로 해석해 볼 수 있다(Baldo & Dronkers, 2006; Birn et al., 2010; Hodges et al., 1992).
VaD의 하위 유형 중 하나인 SVaD는 전임상 단계인 svMCI부터 HC와 대면이름대기 수행력에서 차이를 나타내며 SVaD에서 가장 저하된 수행력을 나타냈다. 생성이름대기의 경우 SVaD가 DAT보다 낮은 수행력을 가지는 것으로 많이 보고되었다. SVaD에서 특징적으로 나타난 생성이름대기의 저하의 경우 과제의 특징과 연관하여 생각해볼 수 있는데, 즉 일상에서 흔히 마주하기 어려운, 흔하지 않고 새로운 자극의 상황을 직면하였을 때 수행력이 저하되는 것은 전두엽 기능장애의 전형적인 패턴으로 나타난다(Han et al, 2006). 따라서 SVaD가 DAT보다 전두엽 기능의 어려움을 더 많이 보이고 있어 생성이름대기 수행력의 저하가 특징적으로 나타나는 것이라고 해석할 수 있다.
VaD의 하위 유형 중 MID를 대상으로 언어 능력을 살펴본 결과, 대면이름대기 능력은 HC와 비교하여 수행력이 저하되나 DAT와 비교하여서는 수행력이 좋은 것으로 나타났다. 이러한 결과는 MID의 경우 반복적인 뇌경색에 의해 전두엽 및 전두엽-피질하 회로가 두드러지게 손상되어 집행기능 측면에서 어려움을 보이고 어휘-의미 지식은 비교적 유지되는 반면(Kertesz & Clydesdale, 1994), DAT의 경우 초기부터 두드러지게 나타나는 측두엽 병변으로 인한 어휘-의미장애가 특징적이기 때문으로 해석해볼 수 있다(Graham et al., 2004).
VaD의 하위 유형 중 CADASIL을 대상으로 언어 능력을 살펴본 결과, 생성이름대기 능력이 HC와 비교하여 CADASIL의 수행력이 저하되었다. 이러한 결과는 CADASIL은 VaD의 아형 중에서 특히 피질하 영역에 국한된 병변과 관련되므로 다른 인지기능 측면보다 특히 전두엽-집행기능의 결함이 두드러지게 나타나는 것(Alexander et al., 1986; Cummings et al., 1994; Ishii et al., 1986)으로 해석된다.
VaD의 하위 유형 중 혼합형 치매(DAT+VaD) 환자를 대상으로 대면이름대기 능력과 청각적으로 설명을 듣고 반응하는 청각적 이름대기 능력을 살펴본 결과, 대면이름대기 및 청각적 이름대기 수행력 모두 혼합형 치매와 VaD가 HC, aMCI, naMCI에 비해 저하되었다. 그러나 혼합형 치매와 VaD 간에는 차이가 관찰되지 않았다. 이는 시각적 처리 과정을 거치는 대면이름대기와 비교하였을 때 청각적 단서를 사용하는 청각적 이름대기 검사는 대면이름대기의 시지각 혼란으로 인한 이름대기 수행력의 저하 등(Petrova et al., 2015)의 단점을 보완하기 때문에 청각적 이름대기가 치매의 이름대기 능력을 더 민감하게 반영할 수 있으므로 대면이름대기와 더불어 청각적 이름대기검사를 함께 실시하는 것이 치매의 이름대기 능력을 확인하는 데 도움이 됨을 시사한다.
본 연구는 VaD 환자를 대상으로 언어 능력을 살펴본 문헌들을 체계적으로 고찰하여 언어의 하위 유형에 따른 특성을 살펴보고자 하였다. 기존의 연구들은 여러 치매 유형의 언어 및 말 유형을 통합적으로 살펴보거나, VaD 환자를 대상으로 하는 경우에도 신경심리학적 측면에 초점을 둔 문헌고찰이 이루어졌다. 이에, 본 연구는 언어병리학적 측면에서 VaD의 언어양식에 따른 세부적 능력을 체계적으로 분석하고 결과를 종합한 최초의 문헌 고찰이라는 점에서 의의가 있다. 또한 VaD의 언어적 특성을 제시함으로써 진단 시 환자의 인지기능 정도와 언어 능력을 함께 고려해볼 수 있는 기초 자료를 제공하였다는 점에서 의의가 있다. 이를 통해 도출된 연구 결론과 그에 따른 제언은 다음과 같다. 첫 번째로, 본 연구는 국내 및 국외 논문을 포함하여 VaD의 언어 특성을 종합하고자 노력하였으나 각 연구마다 제시하는 효과크기가 동일한지에 대한 여부를 살피지는 못하였다는 점에서 한계를 가진다. 추후에는 VaD의 언어 특성에 대한 종합적인 결론에 객관성을 부여할 수 있도록 메타분석이 필요하겠다. 두 번째로, 상당수의 연구가 아형을 분류하지 않고 VaD를 통칭하여 연구를 진행하였음을 알 수 있었다. VaD는 DAT와 같이 동질적(homogeneous)인 다른 유형의 치매들과는 달리 다양한 병인으로 인한 아형들을 총칭하고 있기 때문에(Loeb & Meyer, 1996) 상당히 이질적(heterogeneous)인 집단이라고 알려져 있다(Han et al., 2006;). 그러나 앞서 설명한 바와 같이 VaD 아형들의 병인과 그 병리학적인 기전을 살펴보면 전두엽 회로를 구성하는 대뇌 구조물들을 포함하고 있는 경우가 많기 때문에, 언어 능력에 있어서 서로 다른 아형 간에도 전두엽 기능 저하가 동일한 수준으로 영향을 미치는지 확인할 필요가 있다. 세 번째로, VaD를 포함한 퇴행성 질환 환자들은 중증도에 따라 수행력에 있어 초기 환자의 경우에는 천장효과가, 말기 환자의 경우 바닥 효과가 존재할 가능성이 있으므로 중증도별 연구가 진행될 필요가 있다. 이에 원인뿐만 아니라 중증도에 따른 인지적인 결함 또한 다양하게 나타날 수 있으므로 질환별 특성과 함께 방법적 측면에서 중증도를 고려하는 것이 중요하겠다. 특히 초기 VaD를 정확하게 이해하는 것은 증상을 확인하거나 조기 진단 등에도 필수적이라는 점과 더불어 조기에 진단하여 치료할 경우 더 이상의 진행을 막을 수 있고 호전될 수 있기 때문에 중요하다(Han et al., 2006;). 따라서 각 중증도별 언어 특성을 살피는 것뿐만 아니라 중증도에 따른 언어적 변화를 명확하게 파악하기 위한 종단 연구도 이뤄지는 것이 필요할 것이라고 생각된다. 마지막으로, 언어 하위 유형 중 이름대기 연구가 가장 많았다. 이러한 결과는 VaD가 주로 DAT 집단과의 비교 대상군으로서 연구되었기 때문에 DAT에서 취약한 이름대기 연구가 주로 이루어진 것에 기인한 것으로 생각해볼 수 있다. 또한 다수의 연구가 종합 신경심리검사에 포함된 언어 영역의 결과를 보고하는 형식을 취하였기 때문에, 신경심리검사 내에 포함된 이름대기 항목에 대한 보고가 많이 이루어졌을 가능성이 있겠다. 이에 반하여 특히 따라말하기 연구는 소수에 불과하며, 상반되는 결과가 존재하였기에 그 결과를 종합하기에 다소 어려움이 있었다. 그럼에도 불구하고 문장 따라말하기의 경우, 수행력의 차이를 보고한 연구가 있으므로 이를 보완하여 조금 더 심화적으로 살펴본다면 VaD의 언어 능력을 파악하는 데 많은 도움이 될 것으로 생각된다. 따라서 향후에는 보다 다양한 언어의 하위 영역에서 고른 연구가 이루어져 각 언어 하위 영역마다 VaD의 능력을 자세하게 확인할 수 있기를 기대한다.
Notes
Ethical Statement
N/A
Declaration of Conflicting Interests
There is no conflict of interests.
Funding
This research was supported by Hallym University Research Fund in 2024 (No. HRF-202401-009).
Author Contributions
Conceptualization: Su Min Kwon, Han Sol Lee, Ji Hye Yoon. Data curation: Su Min Kwon, Han Sol Lee. Formal analysis: Su Min Kwon, Han Sol Lee. Investigation: Su Min Kwon, Han Sol Lee. Methodology: Su Min Kwon, Han Sol Lee. Supervision: Ji Hye Yoon. Visualization: Su Min Kwon, Han Sol Lee. Writing—original draft: Su Min Kwon, Han Sol Lee. Writing—review & editing: Ji Hye Yoon. Approval of final manuscript: all authors.
Acknowledgments
N/A
Figure 1.
Flow chart of study selection in the systematic review.
Table 1.
Results of spontaneous speech
Study
Subtype
N
Age (yr)
Education
MMSE
Controls
Tasks
Results
M
SD
M
SD
M
SD
Freitas et al.(2018)
VaD
23
71.7
6.9
9.1
5
-
DAT
ABCD
Object description: HC > VaD, DAT
HC
Concept definition: HC > VaD, DAT
Baillon et al.(2003)
VaD
68
75
-
-
21
-
DAT
Battery of neuropsychological tests
Verbal picture description: VaD > DAT
Bentham et al.(1997)
VaD
10
77.9
6.2
9.7
1.3
17.1
3.9
DAT
Definitions
HC > VaD, DAT
HC
Son & Park(2008)
VaD
40
-
-
-
DAT
Discourse
Total speech quantity: DAT > VaD
Information delivery ability: VaD > DAT
Subject-maintaining ability: result not significant
‘I have no idea’ speech: DAT > VaD
Son & Park(2012)
VaD
40
-
2.5
-
-
DAT
Discourse
A binding sign among groups by VaD severity: mild, moderate, severe > suspected dementia
Vuorinen et al.(2000)
VaD
10
68.4
7
-
20.7
4.4
DAT
Cookie theft picture
Cookie theft picture: HC > VaD, DAT
HC
Object description
Object (orange) description: HC > VaD, DAT
Oh et al.(2010)
VaD
15
79.2
-
1.93
-
17.8
-
DAT
Language tasks involving semantic memory
Verbal definition: VaD > DAT
Villardita(1993)
VaD
30
68.46
6.26
9.6
3.14
-
DAT
Verbal production
The reporter’s test: HC > VaD, DAT
HC
Golden et al.(2005)
VaD
109
78.67
5.35
13.1
2.65
-
DAT
WAIS-R
Information: VaD > DAT
Similarities: VaD > DAT
Vocabulary: result not significant
Nordlund et al. (2007)
vMCI
60
67
7.3
11.2
3.2
28.2
1.8
MCI-nov
WAIS–R
Similarities: HC > vMCI
HC
Powell et al.(1988)
MID
18
67.38
2.45
-
18.77
0.95
DAT
Battery of speech test derived from the Boston Diagnostic Aphasia Examination
Information content: MID > DAT
M: mean, SD: standard deviation, MMSE: Mini-Mental Status Exam, VaD: vascular dementia, DAT: dementia of Alzheimer’s type, HC: healthy control, ABCD: Arizona Battery for Communication Disorders of Dementia, WAIS-R: Wechsler Adult Intelligence Scale-Revised, vMCI: mild cognitive impairment with vascular disease, MCI-nov: mild cognitive impairment with no vascular disease, MID: multiple infarct dementia
Subtests from the standardized finnish version of the Boston Diagnostic Aphasia Examination
Vocabulary comprehension: HC > DAT
HC
Command comprehension: HC > DAT
Comprehension the use of complex tools: HC > VaD, DAT
Villardita(1993)
VaD
30
68.46
6.26
9.6
3.14
-
DAT
Token test
HC > VaD, DAT
HC
Nyström et al.(2015)
vMCI
32
69.2
8.8
10.7
2.4
27.7
1.6
MCI-nov
Token test
Result not significant
HC
Nordlund et al.(2007)
vMCI
60
67
7.3
11.2
3.2
28.2
1.8
MCI-nov
Token test
HC > MCI-nov, vMCI
HC
MCI-nov > vMCI
Traykov et al.(2002)
Subcortical
20
81.2
5
9.5
4.4
23.9
2
DAT
Token test
HC > VaD, DAT
HC
Cannatà et al.(2002)
Subcortical
20
73.1
7.9
7.1
3.4
20.7
3.4
DAT
Token test
HC > s-IVD, DAT
HC
Graham et al.(2004)
Subcortical
19
71.2
7.8
11.6
3.1
25.3
3.8
DAT
Auditory word cognitive test
Word-picture matching: result not significant
HC
Cohen et al.(2002)
Subcortical
24
78.2
5.9
11.9
4
19.9
4.2
HC
Battery of neuropsychological tests
HC > VaD, Subcortical only > cortical + subcortical
Matioli & Caramelli(2012)
Subcortical
13
68
12
7.2
4.9
20.8
3.2
DAT
Battery of neuropsychological tests
Result not significant
HC
Han et al.(2006)
Subcortical
24
67.29
9.38
8.25
3.1
21.04
4.39
DAT
SNSB
SVD > DAT
HC
Emery et al.(1996)
Single cerebral infarction
12
74.8
6.9
12
3.3
21.9
5.1
HC
WAB
Responsive speech: result not significant
Multiple cerebral infarction
17
71.4
7.9
10.7
2.3
22.1
4
Yes/No questions: result not significant
Sentence completion: result not significant
Without cerebral infarction
21
76.9
8.1
11.1
4.2
22.9
5.1
Sequential commands: HC > without > multiple
M: mean, SD: standard deviation, MMSE: Mini-Mental Status Exam, VaD: vascular dementia, DAT: dementia of Alzheimer’s type, HC: healthy control, ABCD: Arizona Battery for Communication Disorders of Dementia, DLB: dementia with Lewy bodies, bvFTD: behavioral variant frontotemporal dementia, lvFTD: language variant frontotemporal dementia, vMCI: mild cognitive impairment with vascular disease, MCI-nov: mild cognitive impairment with no vascular disease, s-IVD: subcortical ischemic vascular dementia, SNSB: Seoul Neuropsychological Screening Battery, SVD: small vessel disease, WAB: Western Aphasia Battery
Table 3.
Results of repetition
Study
Subtype
N
Age (yr)
Education
MMSE
Controls
Tasks
Results
M
SD
M
SD
M
SD
Freitas et al.(2018)
VaD
23
71.7
6.9
9.1
5
-
DAT
ABCD
HC > VaD, DAT
HC
Nordlund et al.(2007)
vMCI
60
67
7.3
11.2
3.2
28.2
1.8
MCI-nov
ASLD logical grammar
HC > vMCI
HC
Vuorinen et al.(2000)
VaD
10
68.4
7
-
20.7
4.4
DAT
Subtests from the standardized finnish version of the Boston Diagnostic Aphasia Examination
Words: result not significant
HC
High probability sentences: HC > DAT
Low probability sentences: HC > DAT
Matioli & Caramelli(2012)
Subcortical
13
68
12
7.2
4.9
20.8
3.2
DAT
Battery of neuropsychological tests
Result not significant
HC
Han et al.(2006)
Subcortical
24
67.29
9.38
8.25
3.1
21.04
4.39
DAT
SNSB
Result not significant
HC
Emery et al.(1996)
Single cerebral infarction
12
74.8
6.9
12
3.3
21.9
5.1
HC
WAB
HC > Single
Multiple cerebral infarction
17
71.4
7.9
10.7
2.3
22.1
4
Without cerebral infarction
21
76.9
8.1
11.1
4.2
22.9
5.1
M: mean, SD: standard deviation, MMSE: Mini-Mental Status Exam, VaD: vascular dementia, DAT: dementia of Alzheimer’s type, HC: healthy controls, ABCD: Arizona Battery for Communication Disorders of Dementia, vMCI: vascular mild cognitive impairment, MCI-nov: mild cognitive impairment with no vascular disease, ASLD: Assessment of Subtle Language Deficits, SNSB: Seoul Neuropsychological Screening Battery, WAB: Western Aphasia Battery
REFERENCES
Ahn, Y., Kim, J. H., Choi, S. H., Jeong, J. H., Ku, B. D., Shim, Y. S., et al. (2016). The difference of verbal fluency task performance between Alzheimer’s disease and subcortical vascular dementia: CREDOS (clinical research Center for Dementia of South Korea) study. Journal of the Korean Neurological Association, 34(1), 14-22.
Alexander, G. E., DeLong, M. R., & Strick, P. L. (1986). Parallel organization of functionally segregated circuits linking basal ganglia and cortex. Annual Review of Neuroscience, 9(1), 357-381.
Assal, F. & Ghika, J. (2013). Language capacities in dementia. Schweizer Archiv für Neurologie und Psychiatrie, 164(8), 280-285.
Baillon, S., Muhommad, S., Marudkar, M., Suribhatla, S., Dennis, M., Spreadbury, C., et al. (2003). Neuropsychological performance in Alzheimer’s disease and vascular dementia: Comparisons in a memory clinic population. International Journal of Geriatric Psychiatry, 18(7), 602-608.
Baldo, J. V. & Dronkers, N. F. (2006). The role of inferior parietal and inferior frontal cortex in working memory. Neuropsychology, 20(5), 529-538.
Barr, A. & Brandt, J. (1996). Word-list generation deficits in dementia. Journal of Clinical and Experimental Neuropsychology, 18(6), 810-822.
Bentham, P. W., Jones, S., & Hodges, J. R. (1997). A comparison of semantic memory in vascular dementia and dementia of Alzheimer’s type. International Journal of Geriatric Psychiatry, 12(5), 575-580.
Birn, R. M., Kenworthy, L., Case, L., Caravella, R., Jones, T. B., Bandettini, P. A., et al. (2010). Neural systems supporting lexical search guided by letter and semantic category cues: A self-paced overt response fMRI study of verbal fluency. Neuroimage, 49(1), 1099-1107.
Braaten, A. J., Parsons, T. D., McCue, R., Sellers, A., & Burns, W. J. (2006). Neurocognitive differential diagnosis of dementing diseases: Alzheimer’s dementia, vascular dementia, frontotemporal dementia, and major depressive disorder. International Journal of Neuroscience, 116(11), 1271-1293.
Brun, A. (1994). Vascular Dementia: Pathological Findings. In Burns, A., Levy, R. Dementia (pp.653-663). Boston, MA: Springer.
Burke, D. M. & Shafto, M. A. (2011). Language and Aging. In Craik, F. I. M., Salthouse, T. A. (3rd ed.). The Handbook of Aging and Cognition (pp.381-451). London: Psychology Press.
Cannatà, A. P., Alberoni, M., Franceschi, M., & Mariani, C. (2002). Frontal impairment in subcortical ischemic vascular dementia in comparison to Alzheimer’s disease. Dementia and Geriatric Cognitive Disorders, 13(2), 101-111.
Canning, S. D., Leach, L., Stuss, D., Ngo, L., & Black, S. (2004). Diagnostic utility of abbreviated fluency measures in Alzheimer disease and vascular dementia. Neurology, 62(4), 556-562.
Carew, T. G., Lamar, M., Cloud, B. S., Grossman, M., & Libon, D. J. (1997). Impairment in category fluency in ischemic vascular dementia. Neuropsychology, 11(3), 400-412.
Chabriat, H., Joutel, A., Dichgans, M., Tournier-Lasserve, E., & Bousser, M. G. (2009). Cadasil. The Lancet Neurology, 8(7), 643-653.
Charidimou, A., Jäger, H. R., & Werring, D. J. (2012). Cerebral microbleed detection and mapping: principles, methodological aspects and rationale in vascular dementia. Experimental Gerontology, 47(11), 843-852.
Chaves, M. L. F., Ilha, D., Maia, A. L. G., Motta, E., Lehmen, R., & Oliveira, L. M. (1999). Diagnosing dementia and normal aging: Clinical relevance of brain ratios and cognitive performance in a Brazilian sample. Brazilian Journal of Medical and Biological Research, 32(9), 1133-1143.
Chenoweth, B. & Spencer, B. (1986). Dementia: The experience of family caregivers. The Gerontologist, 26(3), 267-272.
Chertkow, H., & Bub, D. (1990). Semantic Memory Loss in Alzheimer-Type Dementia. In Schwartz, M. F. Modular Deficits in Alzheimer-Type Dementia (pp.207-244). Cambridge, MA: The MIT Press.
Choi, H. (2008). A comparison of the performances of confrontation naming test and verbal fluency task in patients with prodromal Alzheimer’s disease and mild Alzheimer’s disease. Speech Sciences, 15(2), 111-118.
Choi, H. J. (2015). The relationship between executive function and story comprehension by question type in healthy elderly adults. Journal of Speech-Language and Hearing Disorders, 24(3), 1-13.
Chosak, Reiter J. (2000). Measuring cognitive processes underlying picture naming in Alzheimer’s and cerebrovascular dementia: A general processing tree approach. Journal of clinical and experimental Neuropsychology, 22(3), 351-369.
Clague, F.,, Dudas, R. B., Thompson, S. A., Graham, K. S., & Hodges, J. R. (2005). Multidimensional measures of person knowledge and spatial associative learning: Can these be applied to the differentiation of Alzheimer’s disease from frontotemporal and vascular dementia? Neuropsychologia, 43(9), 1338-1350.
Cohen, R. A., Paul, R. H., Ott, B. R., Moser, D. J., Zawacki, T. M., Stone, W., et al. (2002). The relationship of subcortical MRI hyperintensities and brain volume to cognitive function in vascular dementia. Journal of the International Neuropsychological Society, 8(6), 743-752.
Crossley, M., D’Arcy, C., & Rawson, N. S. (1997). Letter and category fluency in community-dwelling Canadian seniors: A comparison of normal participants to those with dementia of the Alzheimer or vascular type. Journal of Clinical and Experimental Neuropsychology, 19(1), 52-62.
Cummings, J. L. (1998). “Frontal-subcortical circuits and human behavior”: Commentary. Journal of Psychosomatic Research, 44(6), 627-628.
Cummings, J. L., Mega, M., Gray, K., Rosenberg-Thompson, S., Carusi, D. A., & Gornbein, J. (1994). The neuropsychiatric inventory: Comprehensive assessment of psychopathology in dementia. Neurology, 44(12), 2308-2308.
Desmond, D. W. (1994). The neuropsychology of vascular cognitive impairment: Is there a specific cognitive deficit? Journal of the Neurological Sciences, 226(1-2), 3-7.
Dubois, M. F. & Hébert, R. (2001). The incidence of vascular dementia in Canada: A comparison with Europe and East Asia. Neuroepidemiology, 20(3), 179-187.
Ellis, A. W., Young, A. W., & Anderson, C. (1988). Modes of word recognition in the left and right cerebral hemispheres. Brain and Language, 35(2), 254-273.
Emery, V. O. B., Gillie, E. X., & Smith, J. A. (1996). Reclassification of the vascular dementias: Comparisons of infarct and noninfarct vascular dementias. International Psychogeriatrics, 8(1), 33-61.
Er, F., Iscen, P., Sahin, S., Çinar, N., Karsidag, S., & Goularas, D. (2017). Distinguishing age-related cognitive decline from dementias: A study based on machine learning algorithms. Journal of Clinical Neuroscience, 42, 186-192.
Farooq, M. U. & Gorelick, P. B. (2013). Vascular cognitive impairment. Current Atherosclerosis Reports, 15(6), 330.
Federico, A., Di Donato, I., Bianchi, S., Di Palma, C., Taglia, I., & Dotti, M. T. (2012). Hereditary cerebral small vessel diseases: A review. Journal of the Neurological Sciences, 322(1-2), 25-30.
Freitas, M. I. D., Porto, C. S., Oliveira, M. O., Brucki, S. M., Mansur, L. L., Nitrini, R., et al. (2018). Linguistic abilities in major vascular cognitive impairment: A comparative study with Alzheimer’s disease. Acta Neurologica Belgica, 118(3), 465-473.
Gainotti, G., Ferraccioli, M., Vita, M. G., & Marra, C. (2008). Patterns of neuropsychological impairment in MCI patients with small subcortical infarcts or hippocampal atrophy. Journal of the International Neuropsychological Society, 14(4), 611-619.
Garrett, K. D., Browndyke, J. N., Whelihan, W., Paul, R. H., DiCarlo, M., Moser, D. J., et al. (2004). The neuropsychological profile of vascular cognitive impairment--no dementia: Comparisons to patients at risk for cerebrovascular disease and vascular dementia. Archives of Clinical Neuropsychology, 19(6), 745-757.
Giwa, M. O., Williams, J., Elderfield, K., Jiwa, N. S., Bridges, L. R., Kalaria, R. N., et al. (2012). Neuropathologic evidence of endothelial changes in cerebral small vessel disease. Neurology, 78(3), 167-174.
Golden, Z., Bouvier, M., Selden, J., Mattis, K., Todd, M., & Golden, C. (2005). Differential performance of Alzheimer’s and vascular dementia patients on a brief battery of neuropsychological tests. The International Journal of Neuroscience, 115(11), 1569-1577.
Graham, N. L., Emery, T., & Hodges, J. R. (2004). Distinctive cognitive profiles in Alzheimer’s disease and subcortical vascular dementia. Journal of Neurology, Neurosurgery and Psychiatry, 75(1), 61-71.
Gupta, A., Watkins, A., Thomas, P., Majer, R., Habubi, N., Morris, G., et al. (2005). Coagulation and inflammatory markers in Alzheimer’s and vascular dementia. International Journal of Clinical Practice, 59(1), 52-57.
Hachinski, V., Iadecola, C., Petersen, R. C., Breteler, M. M., Nyenhuis, D. L., Black, S. E., et al. (2006). National institute of neurological disorders and stroke-Canadian stroke network vascular cognitive impairment harmonization standards. Stroke, 37(9), 2220-2241.
Hall, J. R., Harvey, M., Vo, H. T., & O’Bryant, S. E. (2011). Performance on a measure of category fluency in cognitively impaired elderly. Aging, Neuropsychology, and Cognition, 18(3), 353-361.
Han, S. K., Ryu, K. H., Kang, Y., Oh., K. J., & Lee, J. H. (2006). Neuropsychological differentiation between mild Alzheimer’s disease and subcortical vascular dementia. Korean Journal of Clinical Psychology, 25(4), 987-1010.
Henskens, L. H., Van Oostenbrugge, R. J., Kroon, A. A., De Leeuw, P. W., & Lodder, J. (2008). Brain microbleeds are associated with ambulatory blood pressure levels in a hypertensive population. Hypertension, 51(1), 62-68.
Herbert, V., Brookes, R. L., Markus, H. S., & Morris, R. G. (2014). Verbal fluency in cerebral small vessel disease and Alzheimer’s disease. Journal of the International Neuropsychological Society, 20(4), 413-421.
Heyanka, D. J., Mackelprang, J. L., Golden, C. J., & Marke, C. D. (2010). Distinguishing Alzheimer’s disease from vascular dementia: An exploration of five cognitive domains. The International Journal of Neuroscience, 120(6), 409-414.
Hier, D. B., Hagenlocker, K., & Shindler, A. G. (1985). Language disintegration in dementia: Effects of etiology and severity. Brain and Language, 25(1), 117-133.
Hirsch, J. A., Cuesta, G. M., Fonzetti, P., Comaty, J., Jordan, B. D., Cirio, R., et al. (2021). Expanded exploration of the auditory naming test in patients with dementia. Journal of Alzheimer’s Disease, 81(4), 1763-1779.
Ho, K. L. & Garcia, J. H. (2000). Neuropathology of the small blood vessels in selected disease of the cerebral white matter. In Pantoni, L., Inzitari, D., Wallin, A. The Matter of White Matter: Clinical and Pathophysiological Aspects of White Matter Disease Related to Cognitive Decline and Vascular Dementia (pp.247-274). Utrecht: Academic Pharmaceutical Productions.
Hodges, J. R., Patterson, K., Oxbury, S., & Funnell, E. (1992). Semantic dementia: Progressive fluent aphasia with temporal lobe atrophy. Brain, 115(Pt 6), 1783-1806.
Ikeda, M., Hokoishi, K., Maki, N., Nebu, A., Tachibana, N., Komori, K., et al. (2001). Increased prevalence of vascular dementia in Japan: A community-based epidemiological study. Neurology, 57(5), 839-844.
Ishii, N., Nishihara, Y., & Imamura, T. (1986). Why do frontal lobe symptoms predominate in vascular dementia with lacunes? Neurology, 36(3), 340-345.
Jang, J. S. & Kim, S. K. (2012). A study on the difference of memory by the types of dementia and utility of CERAD-K to vascular dementia patients. The Journal of Occupational Therapy for the Aged and Dementia, 6(2), 31-38.
Jellinger, K. A. (2013). Pathology and pathogenesis of vascular cognitive impairment-a critical update. Frontiers in Aging Neuroscience, 5, 17.
Johnston, S. C., O’Meara, E. S., Manolio, T. A., Lefkowitz, D., O’Leary, D. H., Goldstein, S., et al. (2004). Cognitive impairment and decline are associated with carotid artery disease in patients without clinically evident cerebrovascular disease. Annals of Internal Medicine, 140(4), 237-247.
Jones, S., Laukka, E. J., & Bäckman, L. (2006). Differential verbal fluency deficits in the preclinical stages of Alzheimer’s disease and vascular dementia. Cortex, 42(3), 347-355.
Kaul, S., Goyal, S., Paplikar, A., Varghese, F., Alladi, S., Menon, R., et al. (2022). Evaluation of vascular cognitive impairment using the ICMR-Neuro Cognitive Tool Box (ICMR-NCTB) in a stroke cohort from India. Annals of Indian Academy of Neurology, 25(6), 1130-1137.
Kertesz, A. & Clydesdale, S. (1994). Neuropsychological deficits in vascular dementia vs Alzheimer’s disease: Frontal lobe deficits prominent in vascular dementia. Archives of Neurology, 51(12), 1226-1231.
Keverne, J. S., Low, W. C. R., Ziabreva, I., Court, J. A., Oakley, A. E., & Kalaria, R. N. (2007). Cholinergic neuronal deficits in CADASIL. Stroke, 38(1), 188-191.
Kim, H., Kang, Y., Yu, K. H., & Lee, B. C. (2015). A comparison of the deterioration characteristics in verbal fluency between amnestic mild cognitive impairment and vascular mild cognitive impairment. Communication Sciences and Disorders, 20(4), 587-595.
Kim, H. J., Ye, B. S., Yoon, C. W., Noh, Y., Kim, G. H., Cho, H., et al. (2014). Cortical thickness and hippocampal shape in pure vascular mild cognitive impairment and dementia of subcortical type. European Journal of Neurology, 21(5), 744-751.
Kim, Y. S. & Shin, M. S. (2014). The comprehension of speech acts ability in Alzheimer’s disease and vascular dementia. Journal of Rehabilitation Psychology, 21(3), 349-372.
Knopman, D. S., Weintraub, S., & Pankratz, V. S. (2011). Language and behavior domains enhance the value of the clinical dementia rating scale. Alzheimer’s and Dementia, 7(3), 293-299.
Korczyn, A. D. (2002). The complex nosological concept of vascular dementia. Journal of the Neurological Sciences, 203, 3-6.
Kugo, A., Terada, S., Ata, T., Ido, Y., Kado, Y., Ishihara, T., et al. (2007). Japanese version of the frontal assessment battery for dementia. Psychiatry Research, 153(1), 69-75.
Kwak, Y. T., Yang, Y., & Kim, G. W. (2010). Korean Addenbrooke’s Cognitive Examination Revised (K‐ACER) for differential diagnosis of Alzheimer’s disease and subcortical ischemic vascular dementia. Geriatrics and Gerontology International, 10(4), 295-301.
Lafosse, J. M., Reed, B. R., Mungas, D., Sterling, S. B., Wahbeh, H., & Jagust, W. J. (1997). Fluency and memory differences between ischemic vascular dementia and Alzheimer’s disease. Neuropsychology, 11(4), 514-522.
Laine, M., Laakso, M., Vuorinen, E., & Rinne, J. (1998). Coherence and informativeness of discourse in two dementia types. Journal of Neurolinguistics, 11(1-2), 79-87.
Laine, M., Vuorinen, E., & Rinne, J. O. (1997). Picture naming deficits in vascular dementia and Alzheimer’s disease. Journal of Clinical and Experimental Neuropsychology, 19(1), 126-140.
Lee, B. T., Kim, K. J., & Cho, M. H. (1996). Comprehension individual differences in reading span and language processing: Working memory and language. Korean Journal of Cognitive and Biological Psychology, 8, 59-85.
Lee, M. J., Seo, S. W., Na, D. L., Kim, C., Park, J. H., Kim, G. H., et al. (2014). Synergistic effects of ischemia and β-amyloid burden on cognitive decline in patients with subcortical vascular mild cognitive impairment. JAMA Psychiatry, 71(4), 412-422.
Lee, S. M., Kim, S. R., & Kim, J. D. (2017). Confrontation naming and verbal fluency of Alzheimer’s disease and vascular dementia. Audiology and Speech Research, 13, 345-351.
Lei, Y., Su, J., Guo, Q., Yang, H., Gu, Y., & Mao, Y. (2016). Regional gray matter atrophy in vascular mild cognitive impairment. Journal of Stroke and Cerebrovascular Diseases, 25(1), 95-101.
Li, M., Meng, Y., Wang, M., Yang, S., Wu, H., Zhao, B., et al. (2017). Cerebral gray matter volume reduction in subcortical vascular mild cognitive impairment patients and subcortical vascular dementia patients, and its relation with cognitive deficits. Brain and Behavior, 7(8), e00745.
Liu, X., Chen, L., Cheng, R., Luo, T., Lv, F., Fang, W., et al. (2019). Altered functional connectivity in patients with subcortical ischemic vascular disease: A resting-state fMRI study. Brain Research, 1715, 126-133.
Loeb, C. & Meyer, J. S. (1996). Vascular dementia: Still a debatable entity? Journal of the Neurological Sciences, 143(1-2), 31-40.
Looi, J. C. & Sachdev, P. S. (1999). Differentiation of vascular dementia from AD on neuropsychological tests. Neurology, 53(4), 670.
Lukatela, K., Malloy, P., Jenkins, M., & Cohen, R. (1998). The naming deficit in early Alzheimer’s and vascular dementia. Neuropsychology, 12(4), 565.
Ma, J., Zhang, Y., & Guo, Q. (2015). Comparison of vascular cognitive impairment-no dementia by multiple classification methods. The International Journal of Neuroscience, 125(11), 823-830.
Marra, C., Ferraccioli, M., Vita, M. G., Quaranta, D., & Gainotti, G. (2011). Patterns of cognitive decline and rates of conversion to dementia in patients with degenerative and vascular forms of MCI. Current Alzheimer Research, 8(1), 24-31.
Marshall, R. S. (2012). Effects of altered cerebral hemodynamics on cognitive function. Journal of Alzheimer’s Disease, 32(3), 633-642.
Matioli, M. N. P. S. & Caramelli, P. (2012). NEUROPSI battery subtest profile in subcortical vascular dementia and Alzheimer’s disease. Dementia and Neuropsychologia, 6(3), 170-174.
McPherson, S. E. & Cummings, J. L. (1996). Neuropsychological aspects of vascular dementia. Brain and Cognition, 31(2), 269-282.
Meyer, J. S., Xu, G., Thornby, J., Chowdhury, M. H., & Quach, M. (2002). Is mild cognitive impairment prodromal for vascular dementia like Alzheimer’s disease? Stroke, 33(8), 1981-1985.
Morris, R. G., Nelis, S. M., Martyr, A., Markova, I., Roth, I., Woods, R. T., et al. (2016). Awareness of memory task impairment versus everyday memory difficulties in dementia. Journal of Neuropsychology, 10(1), 130-142.
Nordlund, A., Rolstad, S., Klang, O., Lind, K., Hansen, S., & Wallin, A. (2007). Cognitive profiles of mild cognitive impairment with and without vascular disease. Neuropsychology, 21(6), 706-12.
Nyström, O., Wallin, A., & Nordlund, A. (2015). MCI of different etiologies differ on the cognitive assessment battery. Acta Neurologica Scandinavica, 132(1), 31-36.
O’Brien, J. (2003). Behavioral symptoms in vascular cognitive impairment and vascular dementia. International Psychogeriatrics, 15(Suppl 1), 133-138.
O’Brien, J. & Thomas, A. (2015). Vascular dementia. The Lancet, 386(10004), 1698-1706.
Oh, H. G., Choi, H., & Kim, S. (2010). Differences of language impairment related to semantic memory in patients with Alzheimer disease and vascular dementia. Journal of Speech and Hearing Disorders, 19(1), 73-84.
Park, J., Kang, Y., Chang, E. J., Oh, E., Yu, K. H., & Lee, B. C. (2006). Clustering and switching on verbal fluency in vascular dementia and dementia of the Alzheimer’s type. Communication Sciences and Disorders, 11(3), 99-112.
Paul, R., Cohen, R., Moser, D., Ott, B., Zawacki, T., & Gordon, N. (2001a). Performance on the Hooper visual organizational test in patients diagnosed with subcortical vascular dementia: Relation to naming performance. Cognitive and Behavioral Neurology, 14(2), 93-97.
Paul, R., Moser, D., Cohen, R., Browndyke, J., Zawacki, T., & Gordon, N. (2001b). Dementia severity and pattern of cognitive performance in vascular dementia. Applied Neuropsychology, 8(4), 211-217.
Peters, N., Opherk, C., Danek, A., Ballard, C., Herzog, J., & Dichgans, M. (2005). The pattern of cognitive performance in CADASIL: A monogenic condition leading to subcortical ischemic vascular dementia. TheAmerican Journal of Psychiatry, 162(11), 2078-2085.
Petersen, R. C., Doody, R., Kurz, A., Mohs, R. C., Morris, J. C., Rabins, P. V., et al. (2001). Current concepts in mild cognitive impairment. Archives of Neurology, 58(12), 1985-1992.
Petersen, R. C., Smith, G. E., Waring, S. C., Ivnik, R. J., Tangalos, E. G., & Kokmen, E. (1999). Mild cognitive impairment: Clinical characterization and outcome. Archives of Neurology, 56(3), 303-308.
Petrova, E. G., Mironov, Y. V., Aoki, Y., Matsushima, H., Ebine, S., Furuya, K., et al. (2015). Comparing the visual perception and aesthetic evaluation of natural landscapes in Russia and Japan: Cultural and environmental factors. Progress in Earth and Planetary Science, 2, 6.
Poore, Q. E., Rapport, L. J., Fuerst, D. R., & Keenan, P. (2006). Word list generation performancein Alzheimer’s disease and vascular dementia. Aging, Neuropsychology, and Cognition, 13(1), 86-94.
Potts, C., Richardson, J., Bond, R. B., Price, R. K., Mulvenna, M. D., Zvolsky, P., et al. (2022). Reliability of Addenbrooke’s Cognitive Examination III in differentiating between dementia, mild cognitive impairment and older adults who have not reported cognitive problems. European Journal of Ageing, 19(3), 495-507.
Powell, A. L., Cummings, J. L., Hill, M. A., & Benson, D. F. (1988). Speech and language alterations in multi‐infarct dementia. Neurology, 38(5), 717-719.
Raimondi, C., Gleichgerrcht, E., Richly, P., Torralva, T., Roca, M., Camino, J., et al. (2012). The Spanish version of the Addenbrooke’s Cognitive Examination-Revised (ACE-R) in subcortical ischemic vascular dementia. Journal of the Neurological Sciences, 322(1-2), 228-231.
Reed, B. R., Mungas, D. M., Kramer, J. H., Ellis, W., Vinters, H. V., Zarow, C., et al. (2007). Profiles of neuropsychological impairment in autopsy-defined Alzheimer’s disease and cerebrovascular disease. Brain, 130(Pt 3), 731-739.
Román, G. C. (1999). Vascular dementia today. Revue Neurologique, 155(Suppl 4), S64-S72.
Román, G. C. & Royall, D. R. (1999). Executive control function: A rational basis for the diagnosis of vascular dementia. Alzheimer Disease and Associated Disorders, 13(Suppl 3), S69-S80.
Román, G. C., Tatemichi, T. K., Erkinjuntti, T., Cummings, J. L., Masdeu, J. C., Garcia, J. H., et al. (1993). Vascular dementia: Diagnostic criteria for research studies: Report of the NINDSAIREN International Workshop. Neurology, 43(2), 250-260.
Roh, E. H. & Park, S. (2019). A comparative study of forms of dementia’s characteristic to improve accuracy of diagnosis of dementia. Health Service Management Review, 13(3), 25-35.
Ross, G. W., Cummings, J. L., & Benson, D. F. (1990). Speech and language alterations in dementia syndromes: Characteristics and treatment. Aphasiology, 4(4), 339-352.
Sachdev, P., Kalaria, R., O’Brien, J., Skoog, I., Alladi, S., Black, S. E., et al. (2014). Diagnostic criteria for vascular cognitive disorders: A VASCOG statement. Alzheimer Disease and Associated Disorders, 28(3), 206-218.
Schmidt, H., Freudenberger, P., Seiler, S., & Schmidt, R. (2012). Genetics of subcortical vascular dementia. Experimental Gerontology, 47(11), 873-877.
Schmidtke, K. & Hüll, M. (2002). Neuropsychological differentiation of small vessel disease, Alzheimer’s disease and mixed dementia. Journal of the Neurological Sciences, 203(-204), 17-22.
Sellal, F., Wolff, V., & Marescaux, C. (2004). The cognitive pattern of vascular dementia and its assessment. In Adamsm, R. J., Awad, I., Bernstein, R., et al. (Vol. 4, No. 2). Seminars in Cerebrovascular Diseases and Stroke (pp.79-86). Philadelphia, PA: WB Saunders.
Smits, L. L., van Harten, A. C., Pijnenburg, Y. A., Koedam, E. L., Bouwman, F. H., Sistermans, N., et al. (2015). Trajectories of cognitive decline in different types of dementia. Psychological Medicine, 45(5), 1051-1059.
Son, E. N. & Park, S. H. (2008). A comparative study of discourse specification on types of dementia. Journal of Special Education and Rehabilitation Science, 47(2), 143-166.
Son, E. N. & Park, S. H. (2012). The characteristics of cohesive device according to the types and degrees of dementia. Journal of Rehabilitation Research, 16(2), 231-247.
Stebbins, G. T., Nyenhuis, D. L., Wang, C., Cox, J. L., Freels, S., Bangen, K., et al. (2008). Gray matter atrophy in patients with ischemic stroke with cognitive impairment. Stroke, 39(3), 785-793.
Tan, L., Xing, J., Wang, Z., Du, X., Luo, R., Wang, J., & et al.. (2023). Study of gray matter atrophy pattern with subcortical ischemic vascular disease-vascular cognitive impairment no dementia based on structural magnetic resonance imaging. Frontiers in Aging Neuroscience, 15, 1051177.
Taylor, A. E., Saint-Cyr, J. A., & Lang, A. E. (1990). Memory and learning in early Parkinson’s disease: Evidence for a “frontal lobe syndrome”. Brain and Cognition, 13(2), 211-232.
Thal, D. R., Grinberg, L. T., & Attems, J. (2012). Vascular dementia: different forms of vessel disorders contribute to the development of dementia in the elderly brain. Experimental Gerontology, 47(11), 816-824.
Traykov, L., Baudic, S., Raoux, N., Latour, F., Rieu, D., Smagghe, A., et al. (2005). Patterns of memory impairment and perseverative behavior discriminate early Alzheimer’s disease from subcortical vascular dementia. Journal of the Neurological Sciences, 229(-230), 75-79.
Traykov, L., Baudic, S., Thibaudet, M. C., Rigaud, A. S., Smagghe, A., & Boller, F. (2002). Neuropsychological deficit in early subcortical vascular dementia: Comparison to Alzheimer’s disease. Dementia and Geriatric Cognitive Disorders, 14(1), 26-32.
Van Straaten, E. C., Scheltens, P., Knol, D. L., Van Buchem, M. A., Van Dijk, E. J., Hofman, P. A., & et al.. (2003). Operational definitions for the NINDS-AIREN criteria for vascular dementia: An interobserver study. Stroke, 34(8), 1907-1912.
Villardita, C. (1993). Alzheimer’s disease compared with cerebrovascular dementia. Neuropsychological similarities and differences. Acta Neurologica Scandinavica, 87(4), 299-308.
Vuorinen, E., Laine, M., & Rinne, J. (2000). Common pattern of language impairment in vascular dementia and in Alzheimer disease. Alzheimer Disease and Associated Disorders, 14(2), 81-86.
Wardlaw, J. M. (2010). Blood-brain barrier and cerebral small vessel disease. Journal of the Neurological Sciences, 299(1-2), 66-71.
Wu, Y., Wang, M., Ren, M., & Xu, W. (2013). The effects of educational background on Montreal Cognitive Assessment screening for vascular cognitive impairment, no dementia, caused by ischemic stroke. Journal of Clinical Neuroscience, 20(10), 1406-1410.
Yeo, H. & Kim, C. M. (2020). Differences in verbal fluencies and discourse comprehension abilities associated with working memory in Alzheimer’s disease and vascular dementia. Journal of the Korea Convergence Society, 11(12), 383-390.
Zhao, Q., Guo, Q., & Hong, Z. (2013). Clustering and switching during a semantic verbal fluency test contribute to differential diagnosis of cognitive impairment. Neuroscience Bulletin, 29(1), 75-82.
APPENDICES
Appendix 1.
Results of naming
Study
Subtype
N
Age (yr)
Education
MMSE
Controls
Tasks
Results
M
SD
M
SD
M
SD
Freitas et al.(2018)
VaD
23
71.7
6.9
9.1
5
-
-
DAT
ABCD
VFT: HC > VaD, DAT
HC
CNT: HC > VaD > DAT
Raimondi et al.(2012)
VaD
32
75.59
6.4
12.97
4.3
-
-
DAT
ACE-R
SFT: DAT > VaD
HC
Smits et al.(2015)
VaD
10
67
5
4.5
2.1
25
4
DAT
Battery of neuropsychological tests
VAT naming: VaD > lvFTD
DLB
ABCD naming: VaD > bvFTD, VaD > lvFTD
bvFTD
SFT: result not significant
lvFTD
PFT: result not significant
HC
Chosak Reiter(2000)
Very mild VaD
25
75.4
7.9
15.8
3.2
28.1
1.5
DAT
BNT
HC > CVD very mild > CVD mild, CVD mod > CVD severe
Mild VaD
30
77.1
8.1
15
3.6
22.9
1.7
HC
Moderate VaD
28
78.6
6.8
10.6
4.3
17.6
1.9
HC > DAT very mild, DAT mild > DAT mod, DAT severe > CVD severe
Severe VaD
14
79.3
5.8
11
4.7
9.7
3.8
Laine et al.(1997)
VaD
10
68.4
7
1.2
0.6
20.7
4.4
DAT
BNT
HC > DAT, HC = VaD, VaD = DAT
HC
Lukatela et al.(1998)
VaD
14
76.7
4.08
11
2.08
24.7
2.73
DAT
BNT
HC > VaD > DAT
HC
Vuorinen et al.(2000)
VaD
10
68.4
7
-
-
20.7
4.4
DAT
BNT
HC > VaD > DAT
HC
Jang & Kim(2012)
VaD
18
65.77
11.21
4.17
4.62
11.78
2.8
DAT
CERAD-K
BNT: DAT > VaD
VFT: result not significant
Braaten et al.(2006)
VaD
31
78.26
4.48
-
-
27.48
2
DAT
BNT
MD, FTD, VaD > DAT
FTD
VFT
PFT: FTD > MDD > VaD
MDD
SFT: FTD, VaD > DAT
Er et al.(2017)
VaD
21
72.09
6.61
9.14
3.59
-
-
ARCD
BNT
ARCD > MCI > DAT > VaD
MCI
VFT
SFT: ARCD > MCI > VaD > DAT
DAT
PFT: ARCD > MCI > DAT > VaD
Heyanka et al.(2010)
VaD
167
79.19
5.57
12.81
2.55
22.5
5.48
DAT
BNT
VaD ≥ DAT
VFT
VaD > DAT
Knopman et al.(2011)
VaD
88
79.6
9.2
13.9
3.7
20.3
7.9
DAT
BNT
DLB > VaD > bvFTD > DAT > PPA
DLB
VFT
bvFTD
Result not significant
PPA
Lafosse et al.(1997)
IVD
32
75.1
10.4
12.6
4.8
22
4
DAT
BNT
Result not significant
VFT
DAT > IVD
Lee et al.(2017)
Mild VaD
10
68.8
-
9.8
-
-
-
DAT
BNT
HC > DAT (mild) > DAT (moderate) > VaD (mild) > VaD (moderate)
Moderate VaD
10
69.3
9.2
HC
VFT
SFT: HC > DAT (mild) > DAT (moderate) > VaD (mild) > VaD (moderate)
PFT: HC > DAT (mild) > DAT (moderate) > VaD (mild) > VaD (moderate)
BNT: HC > VaD, subcortical only > cortical+subcortical
SFT: HC > VaD, subcortical only > cortical+subcortical
Kwak et al.(2010)
Subcortical
42
70.1
10.2
8.6
3.9
20.4
4.6
DAT
K-ACER
VFT: DAT > SIVaD
HC
Peters et al.(2005)
CADASIL
65
47.3
-
10.2
-
27.6
-
HC
Naming
Object: result not significant
Finger: result not significant
VFT
HC > CADASIL
Hirsch et al.(2021)
VaD
83
78.6
7.9
15
2.8
22.7
4
DAT
ANT
HC > VaD, aMCI > VaD, naMCI > VaD
aMCI
HC > mixed, aMCI > mixed, naMCI > mixed
DAT/VaD mixed
128
79.5
6.2
14.2
3
21.9
4.5
naMCI
BNT
HC > VaD, aMCI > VaD, naMCI > VaD
HC
HC > mixed, aMCI > mixed, naMCI > mixed
Chaves et al.(1999)
Multi-infarct
13
-
-
-
-
18.9
6.85
DAT
BNT
HC > MID > DAT
HC
Powell et al.(1988)
MID
18
67.38
2.45
-
-
18.77
0.95
DAT
Naming
MID > DAT
Emery et al.(1996)
Single cerebral infarction
12
74.8
6.9
12
3.3
21.9
5.1
HC
BNT
HC > single, without, multiple
Multiple cerebral infarction
17
71.4
7.9
10.7
2.3
22.1
4
Without = single, without = multiple
Without cerebral infarction
21
76.9
8.1
11.1
4.2
22.9
5.1
WAB
SFT: HC > single, without, multiple,
Without = single, without = multiple
M: mean, SD: standard deviation, MMSE: Mini-Mental Status Exam, VaD: vascular dementia, DAT: dementia of Alzheimer’s type, HC: healthy control, ABCD: Arizona Battery for Communication Disorders of Dementia, VFT: verbal fluency test, CNT: confrontation naming test, ACE-R: Addenbrooke’s Cognitive Examination-Revised, SFT: semantic fluency test, DLB: dementia with lewy bodies, bvFTD: behavioral variant frontotemporal dementia, lvFTD: language variant frontotemporal dementia, PFT: phonemic fluency test, BNT: Boston Naming Test, CVD: cerebrovascular dementia, CERAD-K: The Korean Version of Consortium to Establish a Registry of Alzheimer’s Disease, FTD: frontotemporal dementia, MDD: major depressive disorder, ARCD: age-related cognitive decline, MCI: mild cognitive impairment, PPA: primary progressive aphasia, IVD: ischemic vascular dementia, vMCI: vascular MCI, MCI-nov: MCI with no vascular disease, GNT: Graded Naming Test, VCIND: vascular cognitive impairment no dementia, MoCA: Montreal Cognitive Assessment, CIND: cognitive impairment no dementia, WAIS-R: Wechsler Adult Intelligence Scale-Revised, SVDCI: small vessel disease cognitive impairment, SVD: small vessel disease, E-vMCI: early-vascular MCI, L-vMCI: late-vascular MCI, E-amMCI: early-amnestic multi-domain MCI, L-amMCI: late-amnestic multi-domain MCI, SVCI: subcortical vascular cognitive impairment, SIVD-NCI: subcortical ischemic vascular disease-normal cognitive impairment, SIVD-VD: subcortical ischemic vascular disease-vascular dementia, R-CVD: risk for cerebrovascular disease, svMCI: subcortical vascular MCI, SVaD: subcortical vascular dementia, aMCI: amnestic MCI, PiB: Pittsburgh Compound B, FFT: famous face test, fvFTD: frontal variant frontotemporal dementia, s-IVD: subcortical IVD, SNSB: Seoul Neuropsychological Screening Battery, K-ACER: Korean Addenbrooke’s Cognitive Examination Revised, SIVaD: subcortical ischemic vascular dementia, CADASIL: cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy, ANT: auditory naming test, naMCI: non-amnestic MCI, MID: multiple infarct dementia, WAB: Western Aphasia Battery.
* The scores of Montreal Cognitive Assessment
Appendix 2.
List of 69 articles that were finally selected and analyzed
First author (yr)
Title
Ahn(2016)
The difference of verbal fluency task performance between Alzheimer’s disease and subcortical vascular dementia: CREDOS (Clinical Research Center for Dementia of South Korea) study
Baillon(2003)
Neuropsychological performance in Alzheimer’s disease and vascular dementia: comparisons in a memory clinic population
Barr(1996)
Word-list generation deficits in dementia
Bentham(1997)
A comparison of semantic memory in vascular dementia and dementia of Alzheimer’s type
Braaten(2006)
Neurocognitive differential diagnosis of dementing diseases: Alzheimer’s dementia, vascular dementia, frontotemporal dementia, and major depressive disorder
Cannatà(2002)
Frontal impairment in subcortical ischemic vascular dementia in comparison to Alzheimer’s disease
Canning(2004)
Diagnostic utility of abbreviated fluency measures in Alzheimer disease and vascular dementia
Carew(1997)
Impairment in category fluency in ischemic vascular dementia
Chaves(1999)
Diagnosing dementia and normal aging: Clinical relevance of brain ratios and cognitive performance in a Brazilian sample
Chosak(2000)
Measuring cognitive processes underlying picture naming in Alzheimer’s and cerebrovascular dementia: A general processing tree approach
Clague(2005)
Multidimensional measures of person knowledge and spatial associative learning: Can these be applied to the differentiation of Alzheimer’s disease from frontotemporal and vascular dementia?
Cohen(2002)
The relationship of subcortical MRI hyperintensities and brain volume to cognitive function in vascular dementia
Crossley(1997)
Letter and category fluency in community-dwelling Canadian seniors: A comparison of normal participants to those with dementia of the Alzheimer or vascular type
Emery(1996)
Reclassification of the vascular dementias: Comparisons of infarct and noninfarct vascular dementias
Er(2017)
Distinguishing age-related cognitive decline from dementias: A study based on machine learning algorithms
Freitas(2018)
Linguistic abilities in major vascular cognitive impairment: A comparative study with Alzheimer’s disease
Gainotti(2008)
Patterns of neuropsychological impairment in MCI patients with small subcortical infarcts or hippocampal atrophy
Garrett(2004)
The neuropsychological profile of vascular cognitive impairment—no dementia: comparisons to patients at risk for cerebrovascular disease and vascular dementia
Golden(2005)
Differential performance of Alzheimer’s and vascular dementia patients on a brief battery of neuropsychological tests
Graham(2004)
Distinctive cognitive profiles in Alzheimer’s disease and subcortical vascular dementia
Hall(2011)
Performance on a measure of category fluency in cognitively impaired elderly
Han(2006)
Neuropsychological differentiation between mild Alzheimer’s disease and subcortical vascular dementia
Herbert(2014)
Verbal fluency in cerebral small vessel disease and Alzheimer’s disease
Heyanka(2010)
Distinguishing Alzheimer’s disease from vascular dementia: An exploration of five cognitive domains
Hirsch(2021)
Expanded exploration of the auditory naming test in patients with dementia
Jang(2012)
A study on the difference of memory by the types of dementia and utility of CERAD-K to vascular dementia patients
Jones(2006)
Differential verbal fluency deficits in the preclinical stages of Alzheimer’s disease and vascular dementia
Kaul(2022)
Evaluation of vascular cognitive impairment using the ICMR-Neuro cognitive tool box (ICMR-NCTB) in a stroke cohort from India
Kim(2014)
Cortical thickness and hippocampal shape in pure vascular mild cognitive impairment and dementia of subcortical type
Kim(2014)
The comprehension of speech acts ability in Alzheimer’s disease and vascular dementia
Kim(2015)
A comparison of the deterioration characteristics in verbal fluency between amnestic mild cognitive impairment and vascular mild cognitive impairment
Knopman(2011)
Language and behavior domains enhance the value of the clinical dementia rating scale
Kugo(2007)
Japanese version of the frontal assessment battery for dementia
Kwak(2010)
Korean Addenbrooke’s Cognitive Examination Revised (K‐ACER) for differential diagnosis of Alzheimer’s disease and subcortical ischemic vascular dementia
Lafosse(1997)
Fluency and memory differences between ischemic vascular dementia and Alzheimer’s disease
Laine(1997)
Picture naming deficits in vascular dementia and Alzheimer’s disease
Lee(2014)
Synergistic effects of ischemia and β-amyloid burden on cognitive decline in patients with subcortical vascular mild cognitive impairment
Lee(2017)
Confrontation naming and verbal fluency of Alzheimer’s disease and vascular dementia
Lei(2016)
Regional gray matter atrophy in vascular mild cognitive impairment
Li(2017)
Cerebral gray matter volume reduction in subcortical vascular mild cognitive impairment patients and subcortical vascular dementia patients, and its relation with cognitive deficits
Liu(2019)
Altered functional connectivity in patients with subcortical ischemic vascular disease: A resting-state fMRI study
Lukatela(1998)
The naming deficit in early Alzheimer’s and vascular dementia
Ma(2015)
Comparison of vascular cognitive impairment-no dementia by multiple classification methods
Marra(2011)
Patterns of cognitive decline and rates of conversion to dementia in patients with degenerative and vascular forms of MCI
Matioli(2012)
NEUROPSI battery subtest profile in subcortical vascular dementia and Alzheimer’s disease
Morris(2016)
Awareness of memory task impairment versus everyday memory difficulties in dementia
Nordlund(2007)
Cognitive profiles of mild cognitive impairment with and without vascular disease
Nyström(2015)
MCI of different etiologies differ on the cognitive assessment battery
Oh(2010)
Differences of language impairment related to semantic memory in patients with Alzheimer disease and vascular dementia
Park(2006)
Clustering and switching on verbal fluency in vascular dementia and dementia of the Alzheimer’s type
Paul(2001)
Dementia severity and pattern of cognitive performance in vascular dementia
Paul(2001)
Performance on the Hooper Visual Organizational Test in patients diagnosed with subcortical vascular dementia: Relation to naming performance
Peters(2005)
The pattern of cognitive performance in CADASIL: A monogenic condition leading to subcortical ischemic vascular dementia
Poore(2006)
Word list generation performancein Alzheimer’s disease and vascular dementia
Potts(2022)
Reliability of Addenbrooke’s Cognitive Examination III in differentiating between dementia, mild cognitive impairment and older adults who have not reported cognitive problems
Powell(1988)
Speech and language alterations in multi‐infarct dementia
Raimondi(2012)
The Spanish version of the Addenbrooke’s Cognitive Examination—Revised (ACE-R) in subcortical ischemic vascular dementia
Schmidtke(2002)
Neuropsychological differentiation of small vessel disease, Alzheimer’s disease and mixed dementia
Smits(2015)
Trajectories of cognitive decline in different types of dementia
Son(2008)
A comparative study of discourse specification on types of dementia
Son(2012)
The characteristics of cohesive device according to the types and degrees of dementia
Tan(2023)
Study of gray matter atrophy pattern with subcortical ischemic vascular disease-vascular cognitive impairment no dementia based on structural magnetic resonance imaging
Traykov(2002)
Neuropsychological deficit in early subcortical vascular dementia: comparison to Alzheimer’s disease
Traykov(2005)
Patterns of memory impairment and perseverative behavior discriminate early Alzheimer’s disease from subcortical vascular dementia
Villardita(1993)
Alzheimer’s disease compared with cerebrovascular dementia. Neuropsychological similarities and differences
Vuorinen(2000)
Common pattern of language impairment in vascular dementia and in Alzheimer disease
Wu(2013)
The effects of educational background on Montreal Cognitive Assessment screening for vascular cognitive impairment, no dementia, caused by ischemic stroke
Yeo(2020)
Differences in verbal fluencies and discourse comprehension abilities associated with working memory in Alzheimer’s disease and vascular dementia
Zhao(2013)
Clustering and switching during a semantic verbal fluency test contribute to differential diagnosis of cognitive impairment